
Digital analysis of dental occlusion in just 3 minutes
26 March 2020
Teethan and orthodontics
26 April 2020
The case here was elaborated by Dr. Stefano Montagna and published on Dental Tribune Italian Edition.
Stefano Montagna has a degree in Medicine and Surgery at the University of Parma and is specialized with honors in Odontostomatology at the same University.
Description
A 46-year-old male with complete dentition and a negative history of oral disease. He reported a sensation of “incorrect closing” with occasional difficulty in chewing not well identified. He comes to observation after having made some “retouches to the teeth” that did not improve the sensation of discomfort.Summary of clinical evaluation
The patient reports an uncomfortable dental contact at the left posterior level and diffuse pain on palpation of the muscles of mastication, particularly the lateral pterygoid and posterior digastric muscles. The pain, caused by simple pressure on a muscle, highlights an altered activity of the muscle itself, probably fatigued by an excessive workload.Investigation materials
- Assessment with occlusal maps;- Use of a silicone intra-oral device (Alifix) according to the assessment protocol;
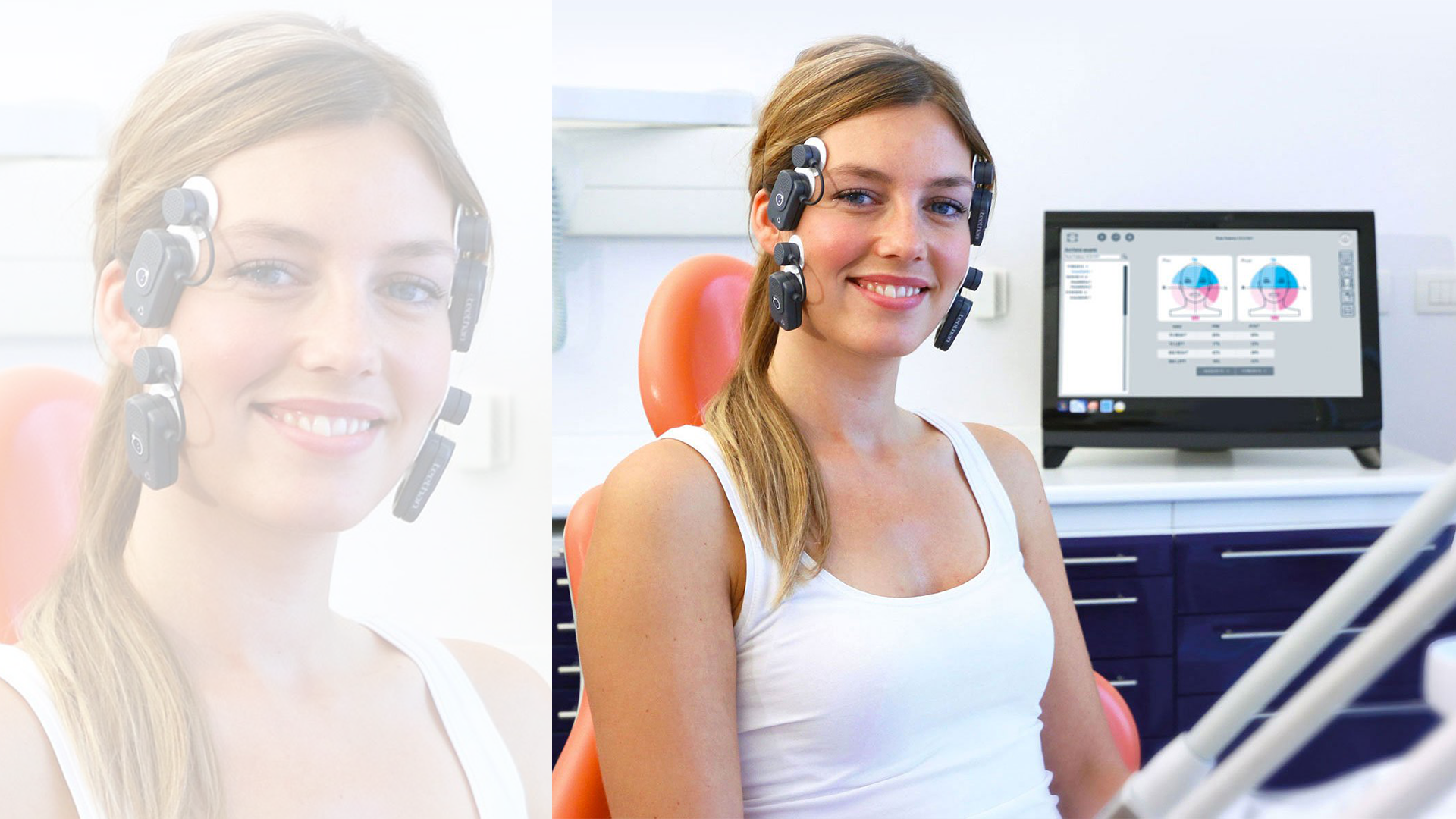
- Surface electromyographic analysis of the Temporal and Masseter muscles according to a standardized protocol (Teethan).
The Alifix device consists of two separate components (right and left) that do not influence each other. Each part is characterized by a vertical element, to be placed on the cheek, and a horizontal, wedge-shaped element, to be inserted between the teeth (Figs. 1, 2). The thicker part of the wedge can be positioned in the anterior or posterior part of the arch and has the function of compensating for any alterations in dental support and providing a homogeneous support condition for muscular rebalancing (1, 2).


Pics 1, 2
The wedge shape of the device allows you to use a proprioceptive stimulus selectively targeted on the Masseter muscle (greater wedge thickness positioned at molar level) or on the temporal muscle (greater wedge thickness positioned at canine-first premolar level) to clinically test muscle activity.
A normal subject, with a well-balanced musculature, does not feel any difference between the position of the greater thickness of the posterior or anterior wedge. If, on the other hand, he/she feels more comfortable with the thicker part of the wedge facing posteriorly, this means that the Masseter muscle has a difficulty in working (often asymptomatic) that is improved by the presence of the wedge thickness; the same is true for the temporal muscle, if the more comfortable position is the one with the thicker wedge positioned anteriorly.
The perception of improvement is clear and immediate, as it exploits the neurological circuit of the reflex arch. The Teethan surface electromyograph allows to detect and compare, through the use of a mathematical algorithm, the simultaneous activity of the Masseter and temporal muscles (3).
A normal subject, with a well-balanced musculature, does not feel any difference between the position of the greater thickness of the posterior or anterior wedge. If, on the other hand, he/she feels more comfortable with the thicker part of the wedge facing posteriorly, this means that the Masseter muscle has a difficulty in working (often asymptomatic) that is improved by the presence of the wedge thickness; the same is true for the temporal muscle, if the more comfortable position is the one with the thicker wedge positioned anteriorly.
The perception of improvement is clear and immediate, as it exploits the neurological circuit of the reflex arch. The Teethan surface electromyograph allows to detect and compare, through the use of a mathematical algorithm, the simultaneous activity of the Masseter and temporal muscles (3).
Investigation procedure
An initial evaluation with occlusal maps confirms the presence of a precontact at the level of the left upper first molar (Fig. 3). An electromyographic analysis of the temporal and masseter muscles is then performed according to a standardized protocol with clamping on the cottons (to eliminate any artifacts) and on the teeth in maximum intercuspation, which shows a muscular imbalance characterized by a prevalent activity of the temporal muscles and an asymmetrical activity of the masseter muscles with greater activity of the left masseter (Fig. 3).
Pic 3
The Alifix device is used according to the recommended protocol:
- The patient should be seated with the backrest elevated;
- Insert Alifix from both sides with the thicker wedge in the posterior position. Have the patient chew and swallow 1-2 times and ask the patient if he/she feels comfortable;
- Repeat the operation placing the thicker wedge anteriorly and ask the patient which of the two positions (thicker wedge in anterior or posterior position) he/she feels more comfortable;
- Report the data on the muscle analysis form.
The patient reports as the most comfortable position the one with the greater thickness of the posterior wedge. The patient is asked to chew and swallow a few times, after which the electromyography is carried out again, this time by having the patient tighten on the device with the thickest wedge positioned bilaterally in the posterior part of the arch (defined by the patient as the most comfortable position).
The presence of the device determines the rebalancing of muscle activity and the electromyographic picture (Fig. 4). Once the device has been removed, the patient is asked to slowly close his mouth and the occlusion is re-evaluated with maps: this time the patient reports a greater posterior contact on the right side (Fig. 4).
- The patient should be seated with the backrest elevated;
- Insert Alifix from both sides with the thicker wedge in the posterior position. Have the patient chew and swallow 1-2 times and ask the patient if he/she feels comfortable;
- Repeat the operation placing the thicker wedge anteriorly and ask the patient which of the two positions (thicker wedge in anterior or posterior position) he/she feels more comfortable;
- Report the data on the muscle analysis form.
The patient reports as the most comfortable position the one with the greater thickness of the posterior wedge. The patient is asked to chew and swallow a few times, after which the electromyography is carried out again, this time by having the patient tighten on the device with the thickest wedge positioned bilaterally in the posterior part of the arch (defined by the patient as the most comfortable position).
The presence of the device determines the rebalancing of muscle activity and the electromyographic picture (Fig. 4). Once the device has been removed, the patient is asked to slowly close his mouth and the occlusion is re-evaluated with maps: this time the patient reports a greater posterior contact on the right side (Fig. 4).

Pic 4
A selective molding of the contact on the right first molar is performed, which is subsequently verified by electromyography that confirms the rebalancing of the electromyographic values and the correspondence with the balance obtained with the Alifix device (R.C. = M.I.) (Fig. 5). Once the selective molding has been performed, the patient reports the disappearance of the sensation of “incorrect closure”.

Fig. 5
Considerations
The use of the Alifix device made it possible to decompensate the muscular system, highlight the difficulty of working the masseters and promote a rebalancing of the muscles. The patient’s sensation of comfort, determined by the posterior position of the wedge, is confirmed by the electromyographic examination.
The balance of the Masseter and Temporal muscles allows you to recover the position of the mandible (R.C.) where the dental contact (M.I.) must be verified, which should be well distributed and without alterations in order to avoid articular overloads. The posterior right contact, not detected by the patient, had probably activated the “avoidance reflex” with retraction and displacement to the left of the mandible. This position, guided by the activation of the Temporal muscles, caused the appearance of contact on the left molar (the one initially perceived by the patient), secondary only to the displacement of the mandible but not the cause of the problem. Taking advantage of the patient’s guidance, with his sensations of balance or unbalance, testing the wedge in different positions, allows us to customize the occlusal rebalancing on that patient.
In addition, the patient is actively involved in the procedure and better understands the problem. This simple procedure of muscular rebalancing, through the use of the Alifix device, inserted as a standardized clinical procedure in the final stages of every dental work before the use of the occlusal maps, allows us to highlight the “real” contact to be eliminated avoiding useless waste of time with continuous retouches made without a guide (4).
Bibliography
1. C. Sforza, S. Montagna, R. Rosati, M. De Menezes. Immediate effect of an elastomeric oral appliance on the neuromuscular coordination of masticatory muscles: a pilot study in healthy subjects. J Oral Rehabil. 2010 37; 840-847.
2. M. Maddalone, E. Bianco, A. Nanussi, G. Costa, M. Baldoni. Treatment of Temporomandibular Disorders of Muscular Origin with a Silicon Oral Device (Alifix®): Electromyographic Analysis. The Journal of Contemporary Dental Practice, 2019 Vol 20 Issue 20; 1367-74.
3. A. Mapelli, G. M. Tartaglia, S. T. Connelly, V.F. Ferrario, C.M. De Felicio, C. Sforza. Normalizing surface electromyographic measures of the masticatory muscles: Comparison of two different methods for clinical purpose. Journal of Electromyography and Kinesiology 30 (2016) 238–242.
4. S.E. Forrester, S.J. Allen, R.G. Presswood, A.C. Toy, M.T.G. Pain. Neuromuscular function in healthy occlusion. J Oral Rehabil. 2010 Sep; 37(9): 663-9.


{kind=link}
{kind=link}
{kind=link}