

Teethan analysis as a tool to implement predictability in Full-Arch implant rehabilitations
13 November 2021
How to prevent orthodontic relapse
22 November 2021
Introduction
The correct evaluation of the DVO represents one of the fundamental aspects for the success of the prosthesis, especially when it comes to implant prosthesis. In fact, a wrong evaluation can compromise the integrity of the prosthetic structures exposing them to an excessive functional load that can determine their breakage. Although DVO plays such an important role, its evaluation is based on non-specific indices such as aesthetics or the clinical need to recover space for prosthetic structures, which certainly have little to do with the patient's muscle work. The role of Teethan in the evaluation of DVO is fundamental as it detects in real time the muscular work of the patient and provides the clinician with the right indices for a correct measurement of the muscular activity.
Case presentation
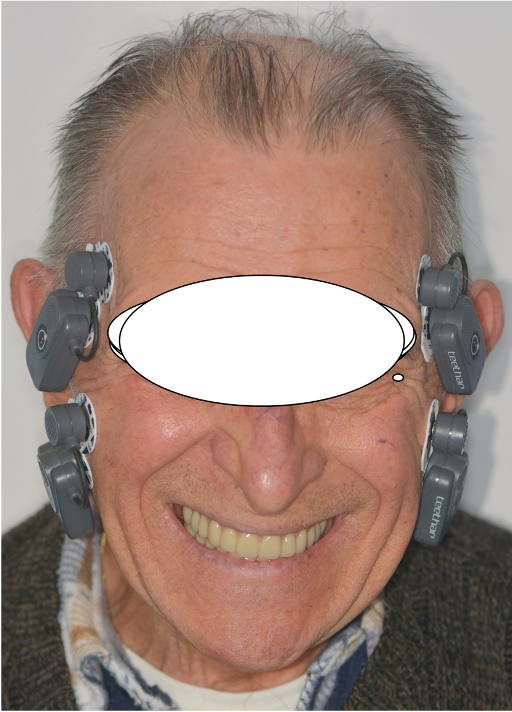
A 78-year-old patient in fair health with an incongruous prosthesis is presented for prosthetic implant rehabilitation.



Treatment
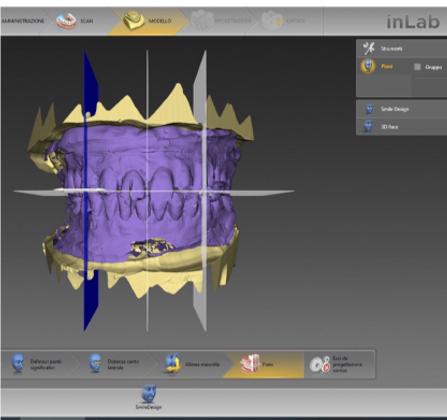
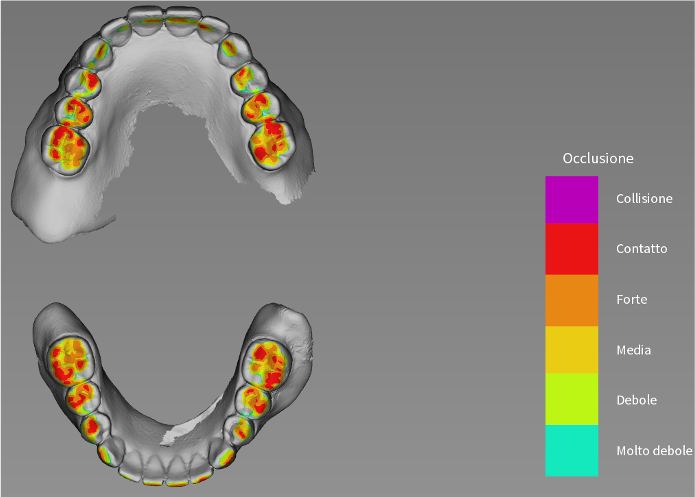
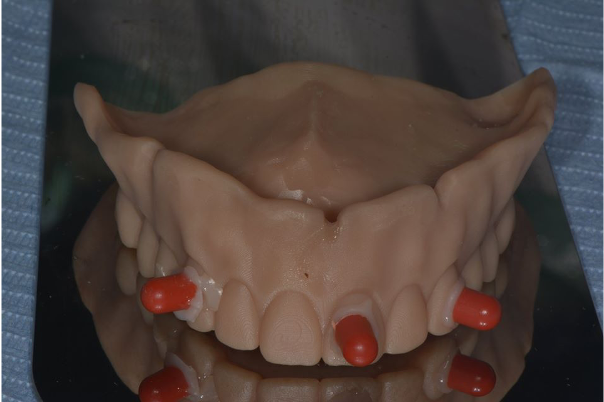
The treatment begins with a baseline assessment of the patient's clinical condition by scanning the prostheses in maximum intercuspation and the subsequent evaluation of the contact points using dedicated software. The scanning of the patient's two prostheses takes place firstly in extra-oral and then intra-oral mode, so that the design of the prosthesis can be fully captured.

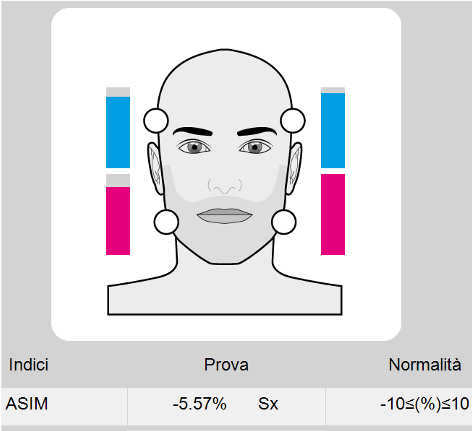
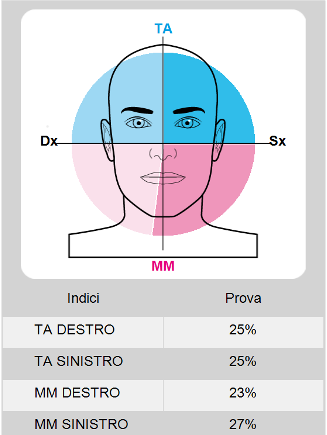
Teethan Exam
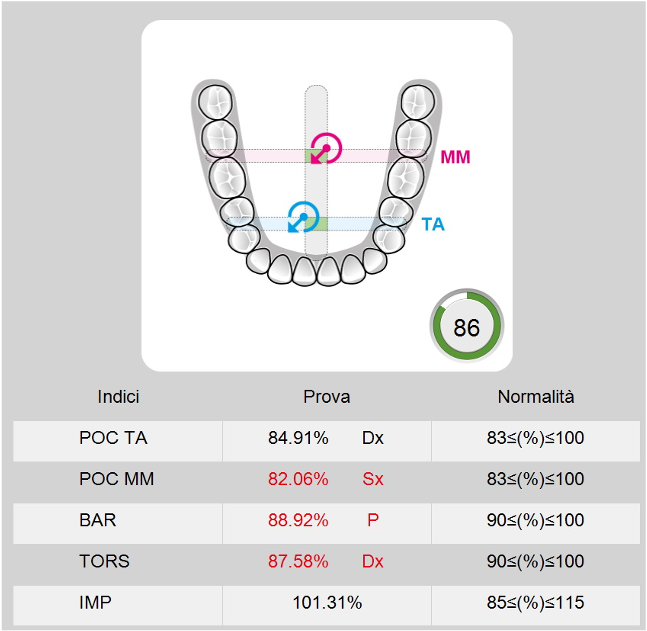
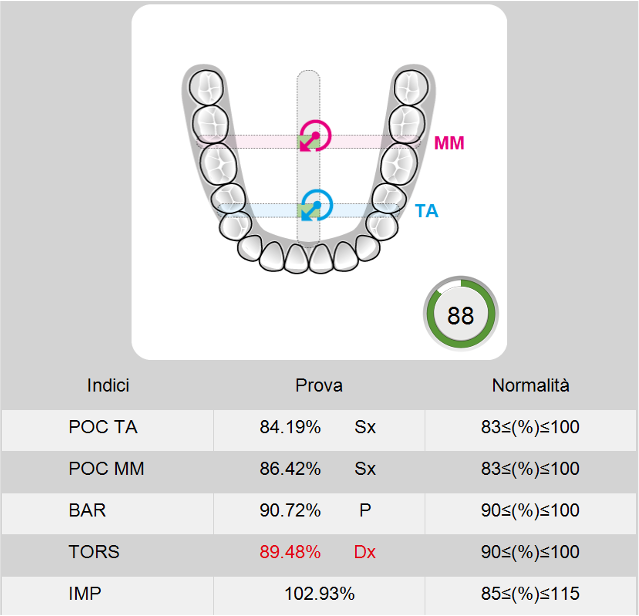
Another very important index in this evaluation phase is the Impact which measures the overall force produced. In this case we have a higher-than-normal Impact index, a sign that we will need to raise the DVO.
Balance correction phase and increase of DVO
From studying the patient's basal condition, we should proceed to balance the occlusion and raise the DVO. Therefore, we will make duplicates of the prostheses molded in resin, so that we can add and remove material without going to modify the original prostheses.
Teethan exam and leaf guage thickness
At this point, by means of a controlled thickness gauge Leaf Gauge, we will add width between the two prostheses to obtain both an occlusal balance and a DVO elevation. The procedure foresees to increase the thickness by reading in real time Teethan data. For convenience, it is better to perform the occlusal balancing first, placing the gauges on one side only. Once Teethan detects a condition of balance, we will proceed to apply constant thicknesses on both sides to raise the DVO. At this point we block out the bite obtained with silicone and scan the prostheses extra-orally again to transfer the precise data to the laboratory.


Prothesis realization
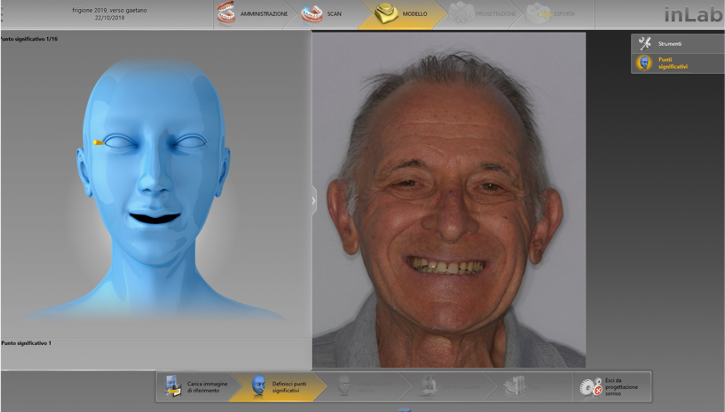
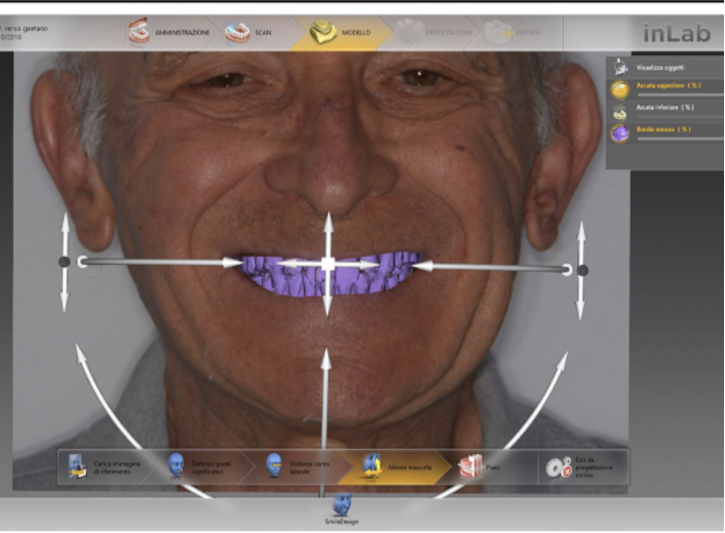
Once scanned the duplicate of the prosthesis with the modifications made, through the digital flow we integrate in the project a facial scan that will optimize the aesthetics and especially adjust the occlusal plane.
Laboratory phase
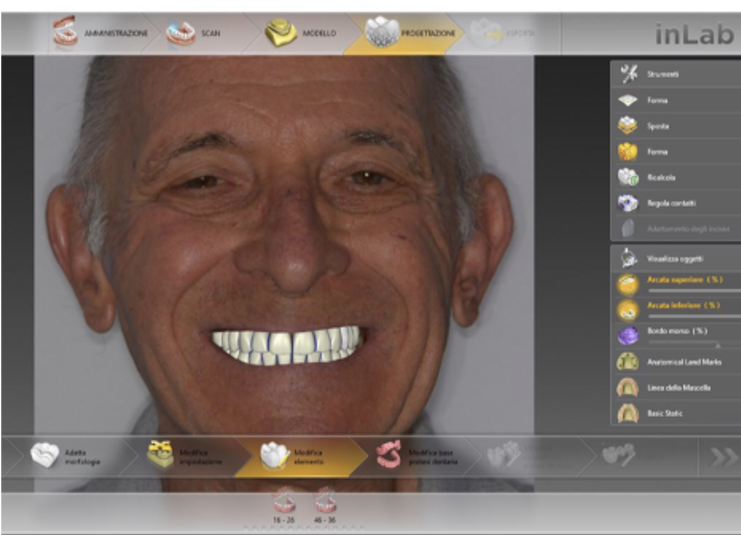
At this point, the team digitally makes the new prosthesis. They consist of two parts, milled in different materials: one for the pink part and one for the teeth. Before delivering the final prosthesis, a single file containing the projects is exported from the software and printed in resin. In this way, it is possible to perform a clinical evaluation of the aesthetics of the prosthesis, but - above all - there will be the possibility to verify in real time both the contact points and the muscle function through Teethan. Moreover, the advantage of the digital flow is being able to make changes on the printed test that can be easily re-scanned and re-entered in the workflow.

Comparing the new Teethan data with the digital analysis of the occlusion we notice that, after redistributing the contacts and raising the DVO, all values tend to stabilize around an Impact index within the average and a better muscular balance. At this stage, radiological landmarks are applied to the printed test and have the patient do the cone beam, so that we can exploit the design of the prosthesis as a virtual wax-up for implant placement within the guided surgery software.

At this point, the mobile prosthesis will be delivered to the patient and used as a functional rehabilitation, with the possibility to – later - make the prosthesis on implants based on the same project.




Surgical treatment
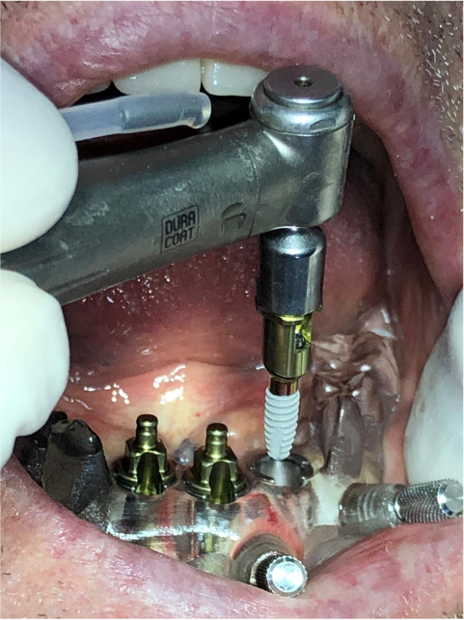
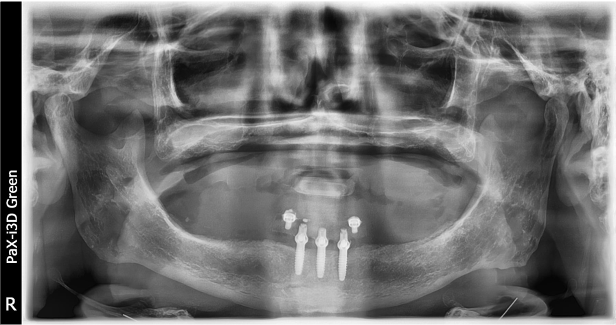
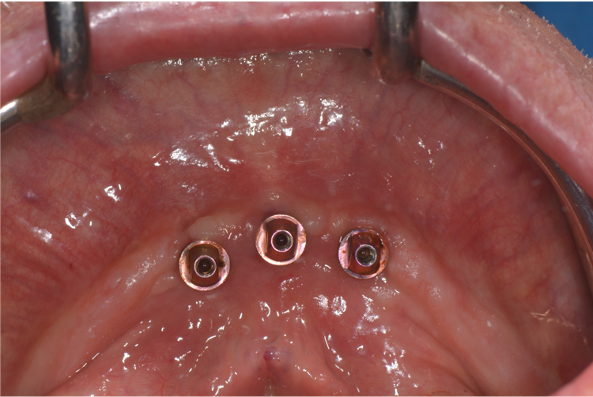
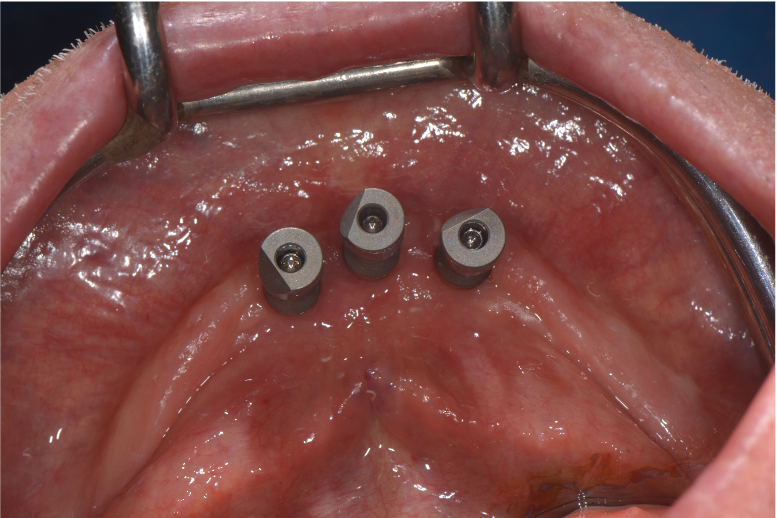
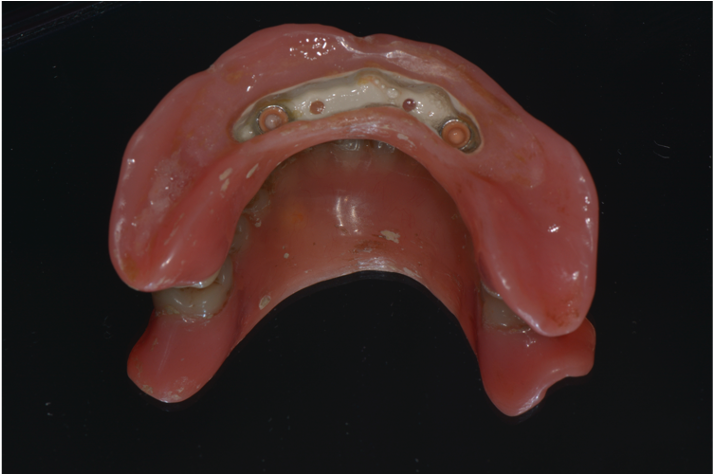
Once the provisional prosthesis is delivered to the patient for functional rehabilitation, the same digital design will be used as a virtual wax-up for prosthetically guided implant placement. This will ensure that the prosthesis, not only distributes the functional load equally, but also has a minimal footprint. Thanks to the guided surgery software the DICOM radiological image of the cone beam will be coupled with the digital project of the prosthesis, that will serve as a virtual wax-up together with the intraoral scan of the patient. Once the implants are virtually positioned, the following step will be to draw the surgical template for the surgery. Following the patient's decision to make implants only from the lower prosthesis, the work was completed with a removable prosthesis fixed on peek bar with the insertion of three lower intraforaminal implants.





Conclusion
- Altered DVO is not a pathology but a clinical condition (if no other TMJ-related pathologies occur, it is always reversible).
- Until now, the assessment of DVO has been based on very non-specific, non-repeatable and operator-dependent indices. Teethan, on the other hand, provides specific indexes, based on the muscular component of TMJ, easily repeatable and independent of the operator.
- The possibility to have a prosthesis made according to the muscular determinants increases the long-term prognosis of implant rehabilitations as it avoids para-functional loads.


{kind=link}
{kind=link}
{kind=link}